


Black women in Maine are far less likely than white women to receive prenatal health care during the course of their pregnancies, and a lack of data about the state’s tribal communities means the racial disparity there may be even worse.
Expecting mothers who are Black are four times more likely than white mothers to go through most or all of a pregnancy without seeing a medical provider, a disparity that is tied with Texas for worst in the country, according to federal data.
The gap is not new but has attracted the attention of the Maine Legislature as the state and the nation confront a wide spectrum of racial inequities, from law enforcement to education, employment and health care.
“These disparities are a public health emergency because decreased access to prenatal care increases the risk of poor health outcomes and even death for both the mother and the child,” Rep. Rachel Talbot Ross, a Democrat from Portland, said in testimony in support of L.D. 1113, a bill being considered by state lawmakers that would direct the Permanent Commission on the Status of Racial, Indigenous and Maine Tribal Populations to study the disparities.
The resolve, sponsored by Sen. Anne Carney, D-Cape Elizabeth, would instruct the commission to analyze the reasons for the disparities – including interviews with impacted women and health care providers – before issuing a report with recommended solutions to create equity in access to prenatal care. The resolve received strong support from the Health and Human Services Committee and faces a full vote by the House and Senate.
The limited data on access to prenatal care clearly show that disparities exist, but the full impact and reasons why are unclear. Health care providers, lawmakers and advocates say they need to better understand why these disparities are happening in order to propose solutions.
Doctors say prenatal care, including regular checkups, ultrasounds and other tests, reduce the risk of complications for both the pregnant woman and her baby and result in better health outcomes after birth. The focus on disparities in access to care for women of color is part of a growing conversation across the United States about health equity and systemic racism in health care.
In Maine, 90 percent of women receive some prenatal care, but there are clear racial disparities in the rates of women who received adequate care. Black women in Maine were four times more likely than white women to go through at least two trimesters without prenatal care in 2019, according to the most recent federal data published in the 2021 Kids Count data book by the Maine Children’s Alliance.
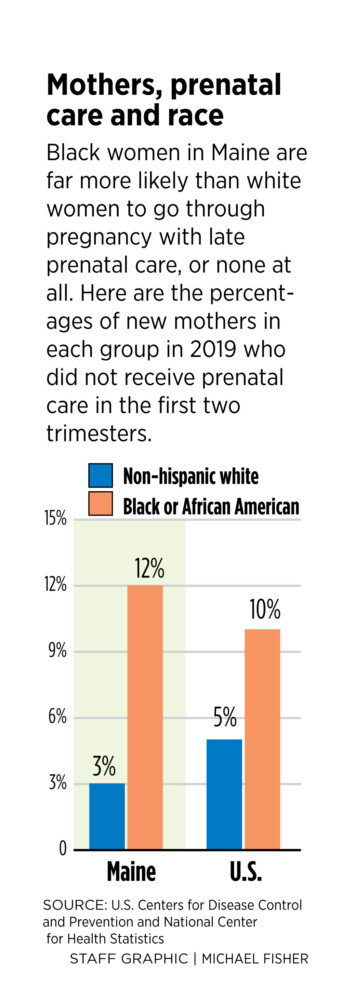
In Maine, 12 percent of Black women did not receive prenatal care until the third trimester or missed out on it entirely. That compares to 3 percent of white women. Overall, 4 percent of all Maine women received prenatal care late, or not at all, in 2019.
The rate for Black women in Maine is higher than the national rate of 10 percent for Black mothers and Maine is tied with Texas for the biggest disparity in rates in the country.
In 2019, a total of 418 women in Maine received late or no prenatal care, including 68 Black women and 17 Hispanic women, according to the Kids Count Data Center from the Annie E. Casey Foundation. Nationally, nearly 233,000 women did not receive prenatal care until later in pregnancy or not at all.
The disparity may be even greater for Indigenous women in Maine, although there are no comparable data.
Nationally, Indigenous women are more likely than any other race category to have delayed prenatal care, with 13 percent of women not receiving care until their third trimester if at all. But the data for Maine do not include a rate for Indigenous women because of a small number of cases, according to the Kids Count Data Center.
Lisa Sockabasin, director of Wabanaki Public Health and a citizen of the Passamaquoddy Tribe at Motahkomikuk, said individuals from communities that experience generational disparities over a long period of time are often misrepresented or not represented in data sets. Maine tribal members have experienced disparities in health care for years, with people sometimes traveling hours away from home for medical appointments, she said.
“When we look at reports like Kids Count or reports the state of Maine might release, oftentimes what we’ll see is an invisibility of populations that are not invisible, that have been present for a long time,” Sockabasin said. “We’re not often asking ourselves the question ‘Who is missing?’ Perhaps the people missing are experiencing the greatest disparities in the state and perhaps even in the United States.”
Carney submitted L.D. 1113 after seeing the data about prenatal care from the Maine Children’s Alliance and learning about the problem at a national conference. Although people have been recognizing and talking about the disparities, it was clear that there wasn’t enough information about why they are happening to propose any kind of solution, she said. The problem is not unique to Maine and other states are looking at it, including Massachusetts, where the state legislature recently passed a bill to form a study commission.
“It’s unclear what is driving these racial disparities in Maine and other states,” said Carney, who has focused as a lawmaker on maternal and children’s health care. “All Mainers should have access to high-quality health care. It’s a basic human right and value we should all share.”
INFANT, MATERNAL MORTALITY
The COVID-19 pandemic and racial justice movement have highlighted longstanding disparities in health and health care for people of color in the United States, including disparities in maternal and infant health that have persisted for years. Maternal and infant mortality rates in the U.S. are higher than other countries of similar wealth.
American Indian/Alaska Native and Black women have rates of pregnancy-related death that are two and three times higher than the rate for white women, according to an analysis by the Kaiser Family Foundation. There are about 700 pregnancy-related deaths in the United States each year, most of which are considered preventable. Cardiovascular conditions are the leading cause of pregnancy-related death.
Black and Indigenous women are more likely to have certain birth risk factors that contribute to infant mortality, and not receiving care until late in pregnancy or at all can increase the risk of complications. They have higher shares of preterm births, low birthweight births or births for which they received no or late care than white women, according to the Kaiser Family Foundation.
From 2014 to 2017, infant mortality among Black women in Maine was 1.4 times higher than the rate for white women, according to a study by the Perinatal System of Care Workgroup published in January 2020. While pointing out the disparity, the study did not delve into the disparity in access to care or impact on infant mortality. Research shows that the disparities exist even when data are controlled for income and education.
“This discrepancy in both maternal and infant health related to race is a national phenomenon,” said Stephanie Eglinton, executive director of the Maine Children’s Alliance. “Obviously there’s a racial discrimination issue that goes beyond other challenges like poverty.”
Dr. Elisabeth Erekson, who chairs the Department of Obstetrics and Gynecology at Maine Medical Center in Portland, said that while it is now known that maternal mortality is significantly influenced by race, more data are needed – especially for Tribal communities – to understand the various reasons for racial disparities in maternal and infant health.
“One of the things that most significantly impacts a good result in pregnancy is having consistent prenatal care throughout the pregnancy. Ensuring that all women have access to high-quality prenatal care throughout their pregnancy helps to result in good outcomes with the pregnancy,” she said. “It’s often the single most modifiable risk factor that we have to help a mom have a good outcome.”
Research shows that insurance coverage increases access to care and that people of color are more likely to be uninsured, as well as face other barriers to care, according to the Kaiser Family Foundation.
Dr. Corrie Anderson, an ob-gyn physician with Northern Light Mercy Women’s Health, said the “huge disparities” in care are a hot topic among doctors nationally as they pay more attention to maternal outcomes.
“Right now, as a community of obstetricians and midwives, we are becoming more aware of these disparities and that we don’t have a great understanding of these disparities,” she said.
Ideally, pregnant women will begin prenatal care by 10 weeks, which allows care providers to ensure they have an accurate estimate of gestational age and due date. Delayed access to prenatal care impacts the ability of doctors to monitor the mother and baby throughout the pregnancy, address medical conditions, screen for abnormalities and connect women with support and resources, Anderson said.
All major medical insurance plans cover pregnancy, including prenatal care, inpatient services, postnatal care and newborn care. These essential services were put in place by the Affordable Care Act, which also made it easier for both planning and expectant mothers to get insurance. Depending on income, pregnant women may qualify for MaineCare, the state’s Medicaid program, which covers prenatal care.
Typically, pregnant women have monthly prenatal appointments early in pregnancy before switching to biweekly appointments at the six-month mark. In the last month of pregnancy, most women have an appointment each week. Women with a history of conditions like high blood pressure and diabetes may see their providers more frequently.
During prenatal appointments, doctors look for maternal health issues like high blood pressure and diabetes so they can intervene early in the pregnancy. Screenings using blood work and ultrasounds will help doctors understand what issues the mother and baby may be experiencing and how to best support the pregnancy and delivery, Anderson said. Throughout the pregnancy, doctors monitor both maternal and infant health.
“The earlier women are establishing care, the better outcomes we’ll have. For many women, it’s the first time they’ll see a doctor since their pediatrician,” Anderson said. “If they present with pre-existing health conditions, then we’re playing catch-up to figure out if it’s something that is pregnancy-related or a baseline maternal condition.”
In Portland, Anderson most often sees delayed access to prenatal care among refugees and asylum seekers. The reasons the woman didn’t receive care sooner are not always clear, but some mothers have not been taught about the importance of presenting for care and how to get it, she said.
“Sometimes it’s just being overwhelmed. It’s just trying to make it one day at a time and taking care of basic needs like housing and food,” she said. “These women astound me in what they go through in coming to a hospital and delivering a baby when you don’t speak their language. It’s such a hurdle to get established care here, then they take that next step to put their babies in someone else’s hands. They say it can be scary.”
At Maine Medical Center, there are a variety of reasons women aren’t accessing prenatal care throughout all trimesters, Erekson said. Some women aren’t familiar with the medical system, while others are significantly limited by times for appointments. The hospital also sees newly arrived immigrants and refugees who have not had access to medical care throughout their pregnancies, she said.
For members of tribal communities, the limited availability of health care in rural areas is a reason some women may not receive adequate care, according to Sockabasin.
“In Washington County and Aroostook County, it is hard to find providers that can provide appropriate care to our women. Oftentimes, the care that our women need, if it is higher-level care, is not offered in our most rural areas. If women aren’t able to seek those services an hour or two hours or more way, what happens?” Sockabasin said. “What is our responsibility as public health and health care professionals to make sure it doesn’t matter where you live in the state, that you have the same chance of having a healthy baby? That it doesn’t matter if you’re Black, brown or Indigenous because you’ll have the same chance? Right now that’s just not the case.”
‘ASYMMETRIC ACCESS’
Carney’s bill about prenatal care disparities drew little attention during a public hearing last month, but advocates for women and children say the legislation is necessary to understand and address the problem.
“We don’t need a special commission to tell us that we have a problem with asymmetric access to prenatal care and outcomes,” said Destie Hohman Sprague, executive director of the Maine Women’s Lobby. “We do need to provide the person power and commitment of a Maine-based commission to provide the dedicated focus that will help us understand where our systems are working and where they can be improved.”
If approved, the legislation would direct the permanent commission to look at the disparities and propose solutions in time for legislation to create equity to be submitted during the second session of the 130th Legislature. During a work session in April, members of the Health and Human Services Committee questioned how that study would be done and if there would be enough time, but ultimately passed the bill out of committee on a 7-2 vote.
The two committee members who did not support the bill, Rep. Michael Lemelin, R-Chelsea, and Rep. Abigail Griffin, R-Levant, said they would support studying access to care for all, but would like to remove all references to race.
Talbot Ross, who chairs the permanent commission, told committee members that the commission last summer identified racial health disparities as a priority for its work and is in strong support of L.D. 1113. Looking at prenatal care disparities would involve reviewing data and speaking with people with lived experience.
Advocates say it is essential to center the voices of people of color as the work is done to better understand the disparities and barriers to care.
“Not only does (this bill) do the deep dive to figure out the barriers to access and how to solve them, but it also includes impacted people as the experts at the table,” Hohman Sprague said. “I think a lot of times we have white-led organizations and white-led systems doing this analysis. The reality is as a white-led organization, I can’t speak to the barriers, but the communities that are experiencing those barriers can. In general, we need to do a better job letting communities and people with the lived experience tell us about what they’re experiencing. Then we need to believe them and act accordingly.”
Sockabasin, from Wabanaki Public Health, said that while the commission should look at disparities in existing data sets, it “must also take on the responsibility of saying, ‘Is this data accurate, what is missing and who is being made invisible?'”
“I think it is imperative that the commission simultaneously look at the data gaps. Basically what they will see is an incomplete picture of reality,” she said. “And they will not get reality until they look at other data sources, like qualitative data sources from the communities that are most impacted.”
Send questions/comments to the editors.

Success. Please wait for the page to reload. If the page does not reload within 5 seconds, please refresh the page.
Enter your email and password to access comments.
Hi, to comment on stories you must . This profile is in addition to your subscription and website login.
Already have a commenting profile? .
Invalid username/password.
Please check your email to confirm and complete your registration.
Only subscribers are eligible to post comments. Please subscribe or login first for digital access. Here’s why.
Use the form below to reset your password. When you've submitted your account email, we will send an email with a reset code.