


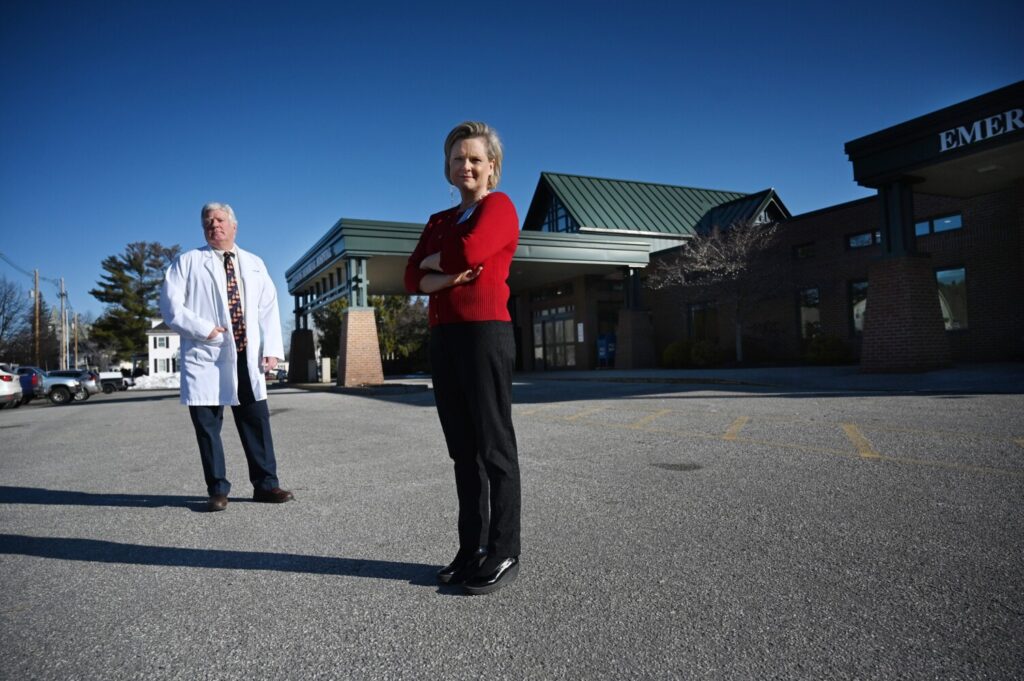
Dr. Greg Hardy, chief medical officer, and Andrea Patstone, Western Maine Healthcare president, photographed outside Stephens Memorial Hospital in Norway, which has postponed all nonessential activity in anticipation of a surge of coronavirus patients. Patstone said, “The hospital is eerily quiet.” Hardy said the 25-bed hospital could have substantially more capacity for COVID-19 patients because of everything it has done to prepare. Shawn Patrick Ouellette/Staff Photographer
Penobscot Valley Hospital in Lincoln opened a coronavirus hotline for patients. Stephens Memorial Hospital in Norway added more than 15 negative pressure rooms to help prevent cross-contamination. Pen Bay Medical Center in Rockport and Waldo County General Hospital in Belfast renovated its Emergency Department waiting rooms to better segregate coronavirus patients from others.
Even though there are not yet widespread cases of coronavirus in small-town Maine, rural hospitals across the state are scrambling to prepare and could be a crucial backstop if Maine’s major hospitals become overrun with coronavirus patients. As of Wednesday, of Maine’s 344 positive COVID-19 cases, 63 were hospitalized, with at least 30 hospitalized in Cumberland County, according to the Maine Center for Disease Control and Prevention.
But the virus is also worsening the financial plight of rural hospitals, many of which are already struggling to survive.
The hospitals are in small towns spread out across Maine, such as Lincoln, Norway, Caribou, Houlton, Calais, Rumford and Dover-Foxcroft. While Cumberland and York counties have combined for 228 of the 303 confirmed COVID-19 cases statewide, officials at the rural hospitals have been using the extra time to prepare for an influx.
To get ready, Maine’s 21 rural hospitals have postponed all nonessential activity – like rehabilitation, routine appointments, physical therapy, elective surgeries, screenings. They’ve shut down much of what they do under normal circumstances – half or more of their operations – as patients who need more complex care are typically transferred to major hospitals.
“We’ve hit the pause button,” said Andrea “Andy” Patstone, president of Western Maine Healthcare, which operates MaineHealth’s Stephens Memorial Hospital in Norway. “The hospital is eerily quiet, like a ghost town.”
Quiet, but prepared, hospital officials said.
“This really highlights the role and importance of rural hospitals,” said Crystal Landry, CEO of the 25-bed Penobscot Valley Hospital in Lincoln, about an hour north of Bangor. “We are prepared for an influx of patients related to COVID-19.”
Maine hospitals are looking to stretch the resources they do have. Maine has 2,893 hospital beds, or 2.5 per 1,000 population, which is slightly above the national average of 2.4 beds per 1,000, according to federal statistics.
Currently, 124 of Maine’s 272 intensive care unit beds are available for use, according to Maine Center for Disease Control and Prevention. About 15-20 percent of all COVID-19 hospitalizations require an ICU bed for the most severely ill, according to experiences in Italy and New York City.
The statewide counts of ICU beds and ventilators reflect an ongoing effort by the Maine CDC and the Maine Hospital Association to gather statewide data on hospital capacity, said Steven Michaud, president of the hospital association.
“It’s called surge planning,” Michaud said. “Should we get hit with a surge of COVID-19 patients, we need to know, for instance, where all the hospital beds, ICU beds and ventilators are at.”
He said the number of ICU beds has grown both because there’s a better accounting of the total statewide beds by Maine CDC and because hospitals are converting more rooms to ICU rooms. An ICU room would have a ventilator and more monitoring equipment for patients. Earlier this week, the statewide capacity of ICU beds was 190, but now it stands at 272.
If 40 percent of Mainers are infected with novel coronavirus within a year – the middle-of-the-road projection by Harvard Global Health Initiative – Maine hospitals will suffer from a critical shortage of hospital beds. The Portland area would need to increase hospital bed capacity by 97 percent, while a 73 percent increase would be needed in the Bangor area.
But the statistical models do not take into account efforts to free up existing space and build more capacity. For instance, officials at MaineHealth’s Stephens Memorial Hospital have increased the number of negative pressure rooms – rooms that are designed to prevent infection spread in hospitals – from two to about 20.
Hospitals are also reassigning and training employees from other disciplines – such as family medicine – to get them ready for COVID-19 patients.
Dr. Gregory Hardy, chief medical officer at Stephens Memorial, said that although Stephens is a 25-bed hospital, its capacity could potentially be substantially higher for COVID-19 because of everything it has done to prepare for the surge. He said it’s difficult to say how much extra capacity it would have, because it depends on how ill the patients are when they are being cared for at Stephens Memorial. MaineHealth – the parent company of Maine Medical Center – operates nine hospitals across the state.
As of right now, all of Maine’s rural hospitals have ventilators and an adequate supply of protective equipment, such as masks, gloves and shoe coverings, needed to take care of COVID-19 patients, according to the Maine Hospital Association. Statewide, Maine’s hospitals have 348 ventilators.
Dr. Nirav Shah, director of the Maine CDC, has said he is extremely concerned about the supply of protective gear for healthcare workers as case numbers climb. While rural hospitals may have an adequate supply now, if the surge occurs that may not continue to be the case.
FINANCIAL HIT
But at the same time rural hospitals have retooled existing resources, they are also seeing sharp revenue declines. The rural hospitals – often in a financially precarious position, especially if they are one of Maine’s nine independent rural hospitals and not part of a larger network – are forgoing revenue from elective procedures.
Michaud said while rural hospitals are readying for patients in case of a surge, they are taking a financial hit. A $100 billion rescue package was approved by Congress last week, but it’s uncertain if it will be enough, Michaud said.
“I am terrified of the financial implications for these hospitals. They are running out of cash right now,” Michaud said. Across the country, 120 rural hospitals have closed since 2010, according to Becker’s Hospital Review. In Maine, hospitals in Brunswick and Boothbay Harbor were converted into other medical services – such as an urgent care center in Boothbay Harbor – when they merged with other health systems.
The United States now has the most confirmed cases of COVID-19 in the world, with more than 205,000 infected people, and has had more than 4,500 deaths. New York City is in crisis mode, and much of the country, including Maine, has shut down schools, businesses and prohibited large gatherings – physical distancing strategies aimed at slowing the spread of the virus.
But if physical distancing efforts don’t stem the tide of cases in Maine in the upcoming weeks, the hospitals in the state’s less-populated areas in western, central, Down East and northern Maine would provide extra capacity if hospitals in larger population centers like Portland, Bangor and Lewiston become overrun with patients.
The hospitals could serve as surge capacity in a number of ways. For instance, a major hospital such as Maine Medical Center could transfer COVID-19 patients to its more rural hospitals in its network, such as Stephens Memorial Hospital, if capacity at Maine Med becomes scarce. People in the community with COVID-19 could also go to their local hospital instead of seeking care in Maine’s larger cities.
SURGE PROTECTORS
Shah said people with COVID-19 do not require complicated care, even though the disease can be life-threatening, so rural hospitals are capable of providing treatment for many patients. The hospitals provide supportive respiratory care with oxygen or a ventilator, giving patients time for their immune systems to fight off the virus.
“Any hospital can manage an individual with COVID-19,” Shah said.
Also, the rural hospitals could serve as “swing beds,” Landry said, which are used for when patients have started to recover but still require hospitalization. A COVID-19 patient who lives closer to Lincoln, for instance, could be transferred out of Northern Light Eastern Maine Medical Center Bangor to be cared for at Penobscot Valley Hospital for the last few days of hospitalization before being sent home.
Erika Ziller, assistant professor of public health at the University of Southern Maine and director of the university’s Rural Health Research Center, said that while rural hospitals have resources, many are in a “precarious financial position” and are often dealing with workforce shortages.
Ziller said rural Maine residents are more likely to be older and sicker with more underlying chronic conditions, so if they do end up hospitalized with COVID-19, they may be more severely ill when they arrive at the hospital. Many would face long drives to get to hospitals, and if they live in Washington of Piscataquis counties, none of the hospitals in those counties has intensive care beds.
While Congress has approved a COVID-19 relief package that includes $100 billion for hospitals, it’s unclear how the money would be doled out, and whether it would arrive in time and would be enough for the most vulnerable rural hospitals to survive.
Maine’s rural hospitals have often struggled financially, Calais Regional Hospital recently closing its obstetrics services and ended outpatient cancer care. Both Calais Regional Hospital and Penobscot Valley Hospital have filed for bankruptcy in recent years.
Landry said at Penobscot Valley, revenue is plummeting, and the hospital doesn’t have a lot of cash reserves.
“When we postpone elective surgeries and screenings, we are decreasing our revenue. We evaluate our finances week to week,” Landry said.
While Maine still has nine remaining independent hospitals, the overall trend is to join a network, such as MaineHealth or Northern Light.
Recently, Mayo Hospital in Dover-Foxcroft joined Northern Light, and Mid-Coast Hospital in Brunswick became part of the MaineHealth network.
Patstone said that being part of MaineHealth gives them financial stability, and they can be part of a centralized planning effort to respond to the COVID-19 crisis.
“I am on a 6 a.m. call with all the MaineHealth hospitals, where we do an inventory of all supplies,” Patstone said. If one hospital is running low, they can move supplies around to other hospitals in the network. “We are part of a network with a systemwide incident command.”
Having enough supplies is crucial to maintaining the workforce needed in case of a surge. If the health care workforce falls ill from COVID-19, not only is it dangerous to them, but it also reduces the capacity of the health care system to care for COVID-19 patients.
The Maine CDC is seeking more protective gear and ventilators as the pandemic becomes more acute across the United States. More creative solutions to potential shortages are being pursued, including manufacturing the protective gear in-state and reconfiguring ventilators so that each ventilator could serve multiple patients.
In New York, they are already splitting ventilators to serve at least two patients for each ventilator. And there’s efforts underway to loan out ventilators from areas that have not yet been hit hard by the pandemic to “hot spots” such as New York, Louisiana and Washington state. When the crisis subsides, the ventilators would be returned or shifted to other parts of the country that need them.
Copy the Story Link
Send questions/comments to the editors.

Success. Please wait for the page to reload. If the page does not reload within 5 seconds, please refresh the page.
Enter your email and password to access comments.
Hi, to comment on stories you must . This profile is in addition to your subscription and website login.
Already have a commenting profile? .
Invalid username/password.
Please check your email to confirm and complete your registration.
Only subscribers are eligible to post comments. Please subscribe or login first for digital access. Here’s why.
Use the form below to reset your password. When you've submitted your account email, we will send an email with a reset code.