


A masked pedestrian walks down Congress Street in Portland. Brianna Soukup/Staff Photographer
As the pandemic summer drew to a close, things looked good for Maine. By almost every metric, the state had kept COVID-19 at bay through the tourist season: Per capita case rates, hospitalizations and deaths were all among the lowest in the country. Five and a half months in, Maine had flattened the curve and then bent it into the ground.
But over the five and a half months that followed, the dam finally broke, spreading the coronavirus to nearly every nook and cranny of Maine. State officials went from reporting a few dozen cases a day to several hundred. Hospitalizations soared to more than 200 at one time, more than triple the worst day of the spring wave. More deaths from the disease were reported in the first two weeks in January than in March, April, May and June combined.
This month there are signs we’ve come out the other side, with case rates, hospitalizations and deaths all headed in the right direction while thousands more Mainers get vaccines with each passing day. But one of the new, super-contagious strains of the virus was detected in the state last week, kicking off a high-stakes race to vaccinate enough Mainers to head off a potentially devastating new surge in the coming weeks.
“Don’t be fooled by the numbers – it’s still all around us,” said Dr. Nirav Shah, the head of the Maine Center for Disease Control and Prevention. “We are still only back in time to where we were in November, not the halcyon days of July and August.”
How did Maine weather this second, more deadly surge, and what did we learn in the process? Top doctors and public health experts say winter weather and holiday gatherings appear to have fueled the massive surge, which has killed 647 Mainers and infected tens of thousands. But the health care system held its ground, hospitals and medical staff got better at treating the pandemic’s victims, and schools and day cares figured out how to stay open without spreading the virus.
Now the challenge will be to keep more contagious forms of the virus in check long enough to get most Mainers vaccinated, stopping its spread.
“It’s a race against time to vaccinate against a spring surge,” said Dr. Dora Anne Mills, chief health improvement officer at MaineHealth, the state’s largest hospital network, and a former director of the Maine CDC. “It won’t be an end-all, but the vaccine is a ticket to the new normal. We won’t be back to life in 2019 – we’ll probably be wearing masks in crowded situations a year or two from now – but individuals will have an extra layer of protection.”
DARK CLOUDS GATHER
At the end of August Mainers also had reason for optimism, even as storm clouds appeared on the horizon.
For weeks, the state had among the lowest per capita new case trends in the country, vying with Vermont and New Hampshire from day to day for the best metrics. For much of July and August, you could count the number of Mainers hospitalized with the disease on two hands, and per capita deaths – 1 per 100,000 – were the lowest in the country, save Vermont. Public health experts say the positivity rate for COVID-19 tests should be under 3 percent; Maine’s rate was down to 0.8.
But public health experts warned that the disease could surge once kids returned to school and colder weather drove social gatherings indoors. Underscoring the disease’s danger, it was already becoming clear that a single ill-advised wedding reception in the Millinocket area had triggered a cascading set of outbreaks across the state.
Presided over by an independent fundamentalist preacher, the Rev. Todd Bell, the Aug. 7 wedding ultimately sickened nearly 200 Mainers, killed at least eight, shut down public schools, locked down a jail and helped push York County – where Bell and many of his congregants lived – into an elevated state of alert. Bell advised his followers to trust in God, not advice from public health experts, to protect them from COVID-19, and he continued hosting maskless services even as the death toll associated with the wedding mounted.
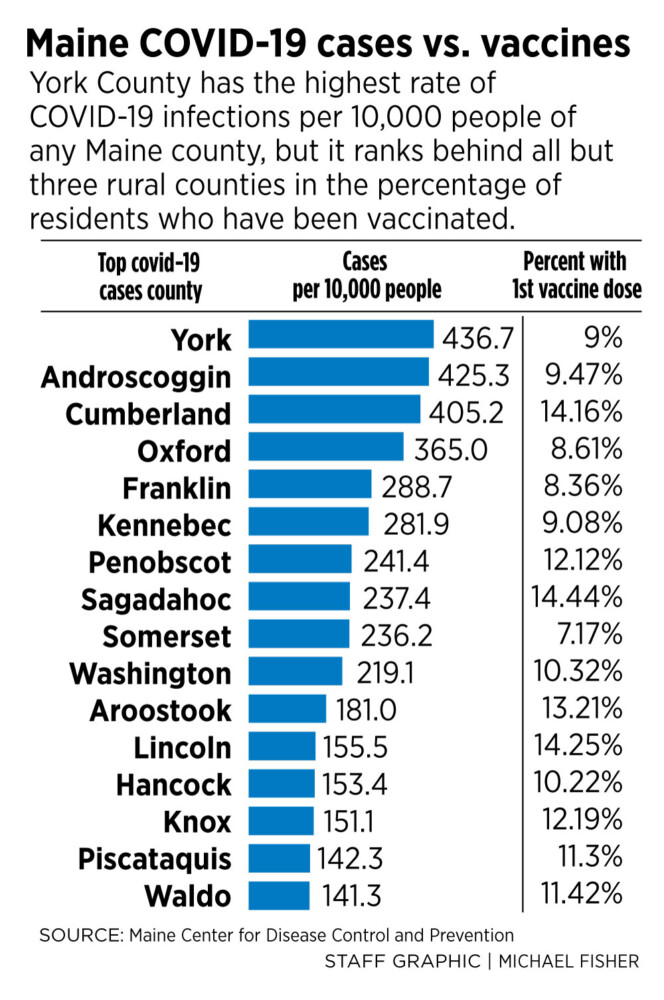
The post-wedding outbreaks put an end to York County’s pandemic hiatus, driving up case counts and making the Sanford area the state’s COVID-19 epicenter for a time. The number of new cases among county residents went from about two a day in mid-August to over 15 in late September, while the daily inpatient count at the county’s largest hospital, Southern Maine Health Care Medical Center, went from near zero to more than five.
“It had a huge effect on York County. We went up to a higher point in new cases that we never really came down from,” says Dr. Evangeline Thibodeau, an infectious disease specialist at York Hospital in York. “It meant we were at a higher level going into the fall surge.”
COVID-19 remained in check across most of the rest of Maine through September and the first half of October, even as many kids returned to at least partial in-person schooling. With masks and other precautions, schools saw almost no transmission of the disease, though by late fall in-person classes were sometimes suspended when a student or teacher who had been exposed in the wider community tested positive for the virus.
“The fear had been that schools would be hotbeds of transmission, but they haven’t,” Shah said. “The risk of in-school transmission (is) more than tolerable – it’s generally speaking as low or lower than just being in the community.”
MaineHealth’s Mills – who is Gov. Janet Mills’ sister – said Maine schools did an excellent job getting personal protective equipment for teachers, staff and students, installing Plexiglas, and devising ways to reduce the risk of in-school exposure. “We had some data that said everything would be OK, but that data was from Denmark and some schools in Georgia that had started earlier,” Mills says. “We were braced for big surges, but fortunately the data was correct.”
Day care centers – whose operation is essential for many working parents – have also turned out to be pretty safe, in part because for some reason small children are poor hosts for the virus. “In day cares, operators are exceedingly risk-averse, so if there is even a hint that someone may theoretically have COVID, they send them home and shut down,” Shah said.
CASE COUNTS RISE
But in nearly every Maine county, new case counts began ticking up noticeably in late October, probably because people were spending more time indoors and cold, dry air makes it easier for coronaviruses to spread.
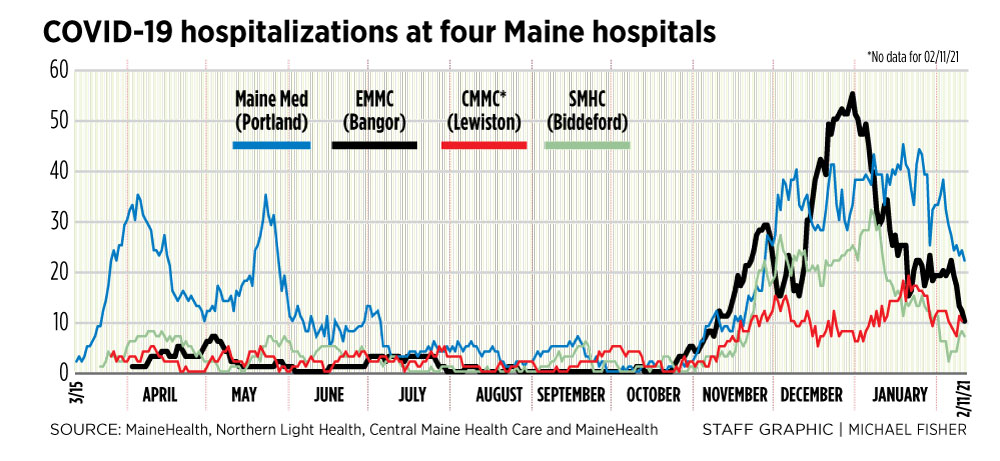
About 6,000 Mainers had gotten the disease between March and Oct. 20, but another 4,000 had tested positive for it a month later and the number of people hospitalized with it had jumped tenfold from nine to 90, with the majority of them in intensive care. This was already 50 percent higher than the heaviest day of the spring surge. For the first time since the pandemic had started, hospitals in Bangor and Augusta – rather than Portland and Lewiston – were the hardest hit.
Until that point, most Maine cases had been associated with outbreaks at long-term care facilities, workplaces, churches and other gathering places. Suddenly many people testing positive had no idea where they had been exposed, and the Maine CDC, stretched thin by the surge, began scaling back contact tracing.
“It was like somebody dropped a whole bunch of salt all around the state,” Mills said. “It was just like everywhere.”
Still, even as the situation deteriorated in Maine, the state was still doing better than the rest of the continental United States. On Nov. 23 it had the second lowest prevalence of the disease in the country after Hawaii.
Models warned worse was coming. They were right.
After more than eight months of social isolation, many Americans decided to spend Thanksgiving with friends and family, despite the risks of travel and indoor, maskless gatherings. This appears to have driven the painfully steep surge of the disease that struck Maine and the United States over the weeks that followed.
In the three weeks following Thanksgiving, the statewide total case count jumped by more than half to over 17,000 while hospitalizations surged from 105 to 187. For reasons that remain unclear, Bangor’s Eastern Maine Medical Center, the hub hospital for the northeastern half of the state, bore the brunt. EMMC, which hadn’t admitted a single COVID-19 patient in the month of September, was caring for 42 three weeks after the holiday and a statewide single-day record of 55 on the last day of December.
But when the post-Christmas COVID-19 tide came in, driving statewide patient counts to record levels by mid-January, it largely spared EMMC. On Jan. 13, the peak day for COVID-19 hospitalizations, there were 207 inpatients statewide, more than triple the spring surge peak of 60. But at EMMC the COVID-19 inpatient count had fallen by almost half to 28, and would fall to under 20 by early February.
“Why it was so regionally affected was the weird thing,” said Dr. James Jarvis, physician incident commander for EMMC’s parent entity, Northern Light Health. “It’s like Thanksgiving hit us hard north of Augusta, but Christmas and New Year’s was particularly hard to the south. Did people in the northern part of the state get scared after Thanksgiving and wore their masks and didn’t travel? We just don’t know.”
Maine’s hospitals endured the January surge remarkably well, and were largely able to avoid postponing elective procedures and other medical services. In early November, computer models had predicted the state might run out of intensive care unit beds, but when they neared capacity, large hospitals like EMMC, Maine Med, MaineGeneral in Augusta and Lewiston’s Central Maine Medical Center expanded capacity by converting “swing beds” in rooms designed to be easily converted to ICUs if needed.
In November, the state’s big three hospital networks – MaineHealth, Northern Light Health, and CMMC parent Central Maine Healthcare – all beefed up the COVID treatment capabilities of their smaller community hospitals so they could treat less acute patients closer to their homes and relieve the burden on their hub medical centers. By design, case counts hit unprecedented levels in January and February at MaineHealth’s PenBay Medical Center in Rockport, CMHC’s Bridgton Hospital and Northern Light’s A.R. Gould Hospital in Presque Isle as the burden was shared out.
For CMHC, making the shift required building new walls and ventilation systems at its Bridgton and Rumford hospitals to make COVID-capable rooms and training staff, said the network’s chief medical officer, Dr. John Alexander. “Patients, especially in smaller communities, want to stay close to home,” he says. “It makes a big difference to know you’re in the town next to where you live, not a city 45 minutes away.”
Jarvis says the shift was also made easier because staff members have become more familiar with how to treat the disease while protecting themselves from it. “Initially we thought we would have to get all these people on a ventilator and breathe for them while they had time to rest,” he said. “Now we’ve found that steroids, oxygen and other therapies are effective, and we’re able to deliver those things in our smaller and critical access hospitals.”
THE SURGE SUBSIDES
The difference in the scale and severity of the spring and winter surges was enormous. A Feb.5 New York Times analysis found Maine had by far the greatest jump in new cases of the 50 states when comparing the seven-day average in early February with the worst week in the spring and summer of 2020: a 461 percent increase. New Hampshire and Vermont – which were also among the best-performing states in the spring and summer – were second and third, at 353 and 238 percent respectively. In Massachusetts and Connecticut, which were harder hit in the first surge, the figure was just 25 percent.
But over the past four weeks, major tracing metrics indicate the surge has let off both in Maine and across the country. By Thursday, Maine hospitalization counts had fallen to their lowest level since before Thanksgiving. On Friday, the seven-day new case average had fallen by two-thirds from its mid-January peak, the lowest level since the beginning of December.
One explanation for the fall is that the Christmas and New Year’s surge has played itself out, though Shah says he distrusts this explanation.
“In pandemic situations, once you achieve a certain threshold of community transmission, usually the curve doesn’t bend – you tend to keep experiencing an increase,” he said. “So what happened? Did everyone in the U.S. decide to start wearing a mask, because I believe just about every county in the country right now has experienced a decline in cases.” He wonders if the dominant strain of the virus has undergone some sort of biological change that accounts for the shift.
Shah also cautions that the road ahead may well be rocky – that we are probably in the eye of the storm, not at the end of it. On Feb. 10 a Franklin County resident with a recent history of overseas travel was found to be carrying the more contagious variant of the virus first identified in the United Kingdom – B.1.1.7 – meaning it has finally arrived in Maine.
In the U.K. and Denmark, the variant quickly became the dominant strain and drove steep surges in the disease, even while Denmark was locked down.
“The more people we can get vaccinated now, the less the virus can circulate and the less chance that the new mutants will get into our population or that new variants will form,” said York Hospital’s Thibodeau. “I think warm weather will help us again, but COVID is here to stay and we’ll have to adapt to it.”
Copy the Story LinkSend questions/comments to the editors.

Success. Please wait for the page to reload. If the page does not reload within 5 seconds, please refresh the page.
Enter your email and password to access comments.
Hi, to comment on stories you must . This profile is in addition to your subscription and website login.
Already have a commenting profile? .
Invalid username/password.
Please check your email to confirm and complete your registration.
Only subscribers are eligible to post comments. Please subscribe or login first for digital access. Here’s why.
Use the form below to reset your password. When you've submitted your account email, we will send an email with a reset code.