

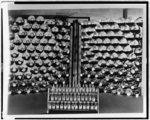
Ampules containing penicillin, with culture bottles which produce the penicillin, in storage in the United States in 1941. Library of Congress
As successful coronavirus vaccine trials dominate headlines across the globe, some politicians continue to treat the effort to end the pandemic as a competitive race between nations.
British officials recently drew the ire of the United States and European Union for fast-tracking approval of the Pfizer-BioNTech vaccine, boasting that the United Kingdom’s early inoculation campaign made it “a much better country” than its European and American rivals. Meanwhile, Pfizer informed U.S. officials that it could not provide significantly more doses of its vaccine than the 100 million already purchased by the United States before next summer, because other countries have bought up its supply.
While this is the most recent example of “vaccine nationalism” — a new term describing unilateral efforts to safeguard domestic interests at the expense of collective ones, as well as the use of such efforts to stoke patriotism — such a stance is hardly unique to Britain. Since March, the United States, China, India, South Korea and Germany, among others, have sought various ways to ring-fence their research, treatments, personal protective equipment and medical equipment.
Some might argue that protecting the nation in times of crisis is precisely what leaders are elected to do. History, however, gives us ample evidence that nationalism is counterproductive when it comes to meeting international medical challenges. Past emergencies suggest that major outbreaks are much more effectively contained through organized collaboration and cooperative diplomacy. When governments treat therapeutic breakthroughs as their exclusive national property, nobody wins.
As a case in point, we need look no further than the most transformative of all 20th-century medical technologies: penicillin. As the catalyst for the entire modern pharmaceutical industry, penicillin tells us much about both the promises and pitfalls of international medical cooperation. And like many of today’s coronavirus vaccines, this revolutionary drug was also once the subject of a transnational crash program.
Library of Congress
The effort had its origins at the University of Oxford during the early years of World War II. There, medical researchers realized that fungal penicillin was so effective at killing bacteria that it might fundamentally alter the treatment of infectious diseases.
The scientists had a problem, however. British factories were not only already working at full capacity for the war effort, they were also being bombed nightly by the Luftwaffe. The only option to develop their breakthrough drug for mass distribution, it seemed, was to work bilaterally with the United States. The decision to share a potentially world-changing discovery with another country was not one to take lightly, but joint development promised to save more lives than either nation might do alone.
The Oxford team set off for the United States, smearing penicillin mold into the lining of their coats in case their flight was intercepted by Nazi saboteurs. Arriving safely in the United States, they settled in at a U.S. Department of Agriculture laboratory in Peoria, Ill., where they joined forces with American fermentation scientists. Although the United States had not yet entered the war, the Peoria scientists quickly understood that the two countries’ pooled knowledge might take penicillin to the next level. Together, the Anglo-American team devised dramatically effective new techniques to isolate, grow and mass-produce the fungus.
So successful were their advances, in fact, that the U.S. government’s main research agency took over the program, creating a medical “Manhattan Project” that brought together the enormous resources of the federal government, the scientific talents of American universities and the production knowledge of private companies such as Merck, Pfizer, Squibb and Lilly.
The U.K. continued sponsoring research on its side of the Atlantic, too, and London shared it freely with the Americans, while British diplomats worked to send new U.S. developments to British firms like Glaxo and Imperial Chemical. The intensity of the challenge and the speed of advancement broke down the usual barriers of national self-interest.
In September 1943, Pfizer converted an old ice factory on Marcy Avenue in Brooklyn into the world’s first commercial penicillin plant. Only nine months later, supplies had grown large enough to meet the needs of the D-Day invasion of Normandy. More than 100,000 Allied soldiers were treated with penicillin, the “miracle” drug that not only made surgeries and amputations less risky, but also freed precious time and resources for field hospitals, doctors and nurses.
Within a year penicillin was available in corner drugstores across the United States and United Kingdom, and soon it began rolling out around the world, subsidized by the Marshall Plan’s postwar reconstruction aid.
Successful transatlantic development of penicillin meant that fatal diseases like pneumonia, scarlet fever and septicemia were treatable. Convalescence time for sexually transmitted diseases and other illnesses was drastically reduced. And a simple prescription from the family doctor could render many dangerous bacterial infections no more harmful to humanity than the common cold.
But if the drug briefly represented a triumph of international collaboration, it also showed the difficulties of maintaining cooperative diplomacy between nations, especially over the sharing of world-changing technologies.
Indeed, penicillin was so transformative that by 1944 Britain and the United States began to quarrel over who had invented it, who should produce it and who should have exclusive rights to it after the war. Bitter diplomatic disputes, professional spats and industrial lawsuits endured well into the 1950s, dashing any hopes of continuing the same kind of far-ranging collaboration in peacetime.
It is not hard to imagine why. Politicians and corporations on both sides of the Atlantic realized that whoever controlled the lifesaving drug would gain enormous geopolitical leverage, not to mention considerable profits. U.S. officials insisted that the millions of research dollars the United States had spent gave it a right to control global distribution. U.K. diplomats insisted that penicillin was “a British discovery which we have made available free to America.”
American firms like Merck filed for penicillin patents in the U.K. and demanded royalties from British companies. U.K. firms accused U.S. ones of violating ethical norms by patenting lifesaving knowledge.
In the end, American officials worked to enforce worldwide monopolies for U.S. pharmaceutical companies, while British policymakers vowed that such an easy giveaway would never happen again. In 1948, Parliament created a new science and technology body, the National Research Development Corporation, to make sure that inventions like penicillin would in the future be exploited by Britain alone. Then as now, nationalist temptations proved difficult to resist.
History thus shows us that in grave emergencies, international cooperation and the rational pooling of resources can lead to astonishing breakthroughs with the potential to save millions of lives. It also shows us that nationalism and the impulse to hoard discoveries by individual countries may impede the ability of science to conduct ongoing collaborations and produce continual improvements that benefit everybody.
Anyone alarmed by the continued global spread of the novel coronavirus should be equally alarmed by the impulse toward “vaccine nationalism.” History reveals that medical crises demand leadership, cooperation and mutual action, with a disregard for national self-interest to match the virus’s own disregard for borders.
As United Nations Director General António Guterres recently declared, “For the first time since 1945, the entire world is confronted by a common threat, regardless of nationality, ethnicity or faith. But while COVID-19 does not discriminate, our efforts to prevent and contain it do.”
If setting nationalism aside helped fuel the lifesaving production of penicillin in the 1940s, there is no reason to allow our political boundaries to prevent respectful, united and fully collaborative science from being put to work for us today.
Falcone is a postdoctoral fellow in the Brady-Johnson Program in Grand Strategy and International Security Studies at Yale University. His research analyzes the role of science and technology in U.S. foreign relations.
Send questions/comments to the editors.

Success. Please wait for the page to reload. If the page does not reload within 5 seconds, please refresh the page.
Enter your email and password to access comments.
Hi, to comment on stories you must . This profile is in addition to your subscription and website login.
Already have a commenting profile? .
Invalid username/password.
Please check your email to confirm and complete your registration.
Only subscribers are eligible to post comments. Please subscribe or login first for digital access. Here’s why.
Use the form below to reset your password. When you've submitted your account email, we will send an email with a reset code.